
Adenoidectomy is the removal of adenoids. Adenoidectomy is a safe and common throat operation.
Swollen or enlarged adenoids are common in children. Causes include:
- Infections with viruses or bacteria. Once an infection clears, the swelling often goes down but sometimes the adenoids remain enlarged.
- Allergies
- Throat infections.
- Recurrent childhood ear disease.
- Often there is no apparent cause.
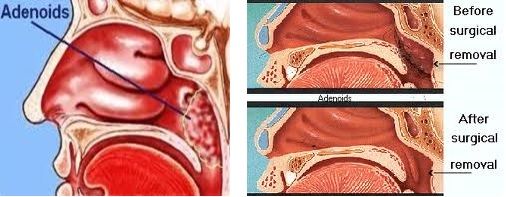
Excision through the mouth
The adenoids are most commonly removed through the mouth after placing an instrument to open the mouth and retract the palate. The adenoids are visualized endoscopically and removed with coblation. This method causes also no bleeding and there is minimal to no post-operative pain.
Excision through the nose
Adenoids may also be removed through the nasal cavity with a surgical suction instrument called a microdebrider endoscopically. With this procedure, bleeding is controlled either with packing or suction cautery. Endoscopic visualization and complete removal is the main advantage of this method.
In rare cases, significant postoperative bleeding may occur. Bleeding usually happens in the first 24 hours after surgery and is short lived.
Adenoidectomy is sometimes performed in conjunction with a tonsillectomy.
Return to daily activities when you feel well enough. Some people are ready in a few days; others may need a whole week. It is recommended that children avoid heavy playground activities, physical education class, or sports teams for two weeks.
Report any bleeding immediately. Bleeding usually happens between seven and 10 days after surgery when the wet scabs in the back of the throat are sloughing off. Ninety-eight percent of the time this is a brief bleed that is not significant.
Call your doctor’s office if you experience any of the following:
- A temperature of more than 102°F
- Ear pain that lasts more than three days or severe ear pain
- Neck pain associated with a stiff neck or fixed head position
- Excessive bleeding
Sometimes medical therapy fails to resolve the chronic tonsillar infections that affect your child. In other cases, your child may have enlarged tonsils, causing loud snoring, upper airway obstruction, and other sleep disorders.
You may be advised to have your tonsils removed in certain situations. In particular:
- If you have frequent and severe bouts of tonsillitis. This usually means:
- Seven or more episodes of tonsillitis in the preceding year.
- Five or more such episodes in each of the preceding two years.
- Three or more such episodes in each of the preceding three years.
- The bouts of tonsillitis affect normal functioning. For example, they are severe enough to make you need time off from work or from school.
- If you have large tonsils that are partially obstructing your airway, this may be a contributing factor to a condition called obstructive sleep apnoea syndrome.
- If you develop cancer of the tonsil.
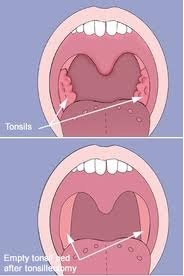
The best recourse for such conditions may be removal or reduction of the tonsils. Children who have three or more tonsillar infections a year undergo a tonsillectomy; the young patient with a sleep disorder should be a candidate for removal or reduction of the enlarged tonsils. Tonsillectomy is one of the most common surgical procedures performed on children. It was also very painful. With the advent of new techniques, the post-operative period for the child is almost pain-free.
Various methods are available for removal of tonsils:
Dissection and Snare method: This is the commonly used method to perform a tonsillectomy, in various parts of the country. The tonsil is dissected along with its capsule and lifted out of its bed. It is ultimately removed using a tonsillar snare. Snaring the tonsil has a distinct advantage. Since the tonsil is crushed before it is cut, bleeding is minimised. The advantage of this method is that the procedure is safe, bleeding is less and the tonsil can be removed in toto without any remnants.
Intracapsular Tonsillectomy: A microdebrider set at 1500 rpm in the oscillating mode is used to perform the intracapsular tonsil resection, and a thin rim of lymphoid tissue was left on the capsule. Suction cautery is used for hemostasis. This results in a decrease in postoperative pain and recovery time as compared to standard tonsillectomy.
Harmonic Scalpel Tonsillectomy: The harmonic scalpel is an ultrasonic dissector coagulator that utilizes ultrasonic vibration to cut and coagulate tissues. The cutting mechanism is possible with the sharp blade with a vibratory frequency of 55.5 kHz over a distance of 89 μm. The coagulation mechanism occurs by transferring mechanical energy to tissues. This breaks hydrogen bonds of proteins and generates heat from tissue friction. The temperature of the harmonic scalpel is lower than electrocautery (50° – 100° C, 150° – 400° C, respectively), and there is less thermal damage to tissues.
Laser Tonsillectomy: The CO2 and KTP lasers have been used to perform tonsil surgery. There is a less postoperative pain, more rapid healing, less blood loss, and less operative time using the CO2 laser. Although the patients have greater difficulty tolerating a diet two and three weeks postoperatively.
Coblation: Coblation, or cold ablation, is a technique that utilizes a field of plasma, or ionized sodium molecules, to ablate tissues. Bipolar radio-frequency energy is transferred to sodium ions, creating a thin layer of plasma. This effect is achieved at temperatures from 40° to 85° C, in comparison to electrocautery which can reach above 400° C. The reduction in thermal injury to surrounding tissues offers reduced postoperative pain and morbidity and an almost bloodless field intraoperatively.

Micro-Laryngeal Surgery is a Minimally Invasive Technique that helps in the correction of the voice disorder or problem in the larynx. It involves the removal of the unwanted and unnatural growth in the larynx such as cysts or polyps that may not respond to more conservative treatment and needs surgery.
Almost all microlaryngeal surgery is done under general anesthesia. The patient must be anaesthetized strongly enough so that he does not gag with the laryngoscope in place.
Microlaryngeal Surgery is extremely safe. Like any surgery, there are some risks. There are slight risks of general anaesthesia, especially in individuals with severe heart or lung problems. Specific risks from the laryngoscope include pain and numbness to the tongue due to pressure (fairly common), some bruising to the lips (also relatively common), and in a worst-case scenario, a chipped tooth (quite rare, but still possible if it is hard to see the vocal folds).
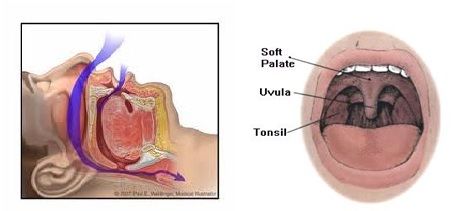
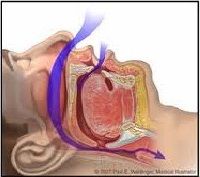
Snoring is caused by vibration of the soft palate (the soft part of the mouth’s roof) as the lungs strain to inhale oxygen through obstructed airways.
Causes
- Poor nasal airflow
- Loose tissues in the throat
- Loose tissues in the roof of mouth – soft palate
- Large tonsils and adenoids
- A large or mispositioned tongue
- Abnormalities in the jaw
- Excess neck fat
Major signs and symptoms of sleep apnea
- Loud and chronic snoring
- Choking, snorting, or gasping during sleep
- Long pauses in breathing
- Daytime sleepiness, no matter how much time you spend in bed
- Waking up with a dry mouth or a sore throat
- Morning headaches
- Restless or fitful sleep
- Insomnia or nighttime awakenings
- Going to the bathroom frequently during the night
- Waking up feeling out of breath
- Forgetfulness and difficulty concentrating
- Moodiness, irritability, or depression
Nasal blockage can be caused by a twist in the nasal septum cartilage. Other nasal problems include swelling of the nasal tissues due to allergy or polyps. If a nasal blockage is part of your snoring problem, this will be your first operation.
Nasal Surgery options for snoring
Radio-frequency Cauterization of Inferior turbinates
Radio-frequency energy can be used to shrink the turbinates by creating scar tissue in them which results in a more open nasal passage. The procedure takes about 15 minutes. Most of that time is spent anaesthetizing the nasal tissue with topical and other anaesthetics injected into the area.
Multiple applications are done on each side of the nose for maximal effect. After the scar tissue is formed, which takes about 3 months; one can notice the full effect of the procedure. The scar tissue will soften over time and the swelling and narrowing may recur. If needed, the procedure can be repeated.
Deviated septum
The septum deviation can be corrected by removing the crooked cartilage. This surgery usually is performed in the operating room under general anaesthesia. After surgery, if the nasal obstruction is improved, the snoring often improves.
Nasal polyps
If the polyps are large enough, they will require surgery to remove them. This is done in an operating room under general anaesthesia. Removing the polyps reduces nasal obstruction, which may improve snoring.
Tonsils and Adenoids
If tonsils and adenoids are enlarged, infected; they could be the cause of snoring in children. Removing the adenoids and tonsils reduces snoring problems especially in children.
Uvulectomy
Uvulectomy is the removal of the uvula. This can easily be performed under local anaesthesia. A person usually does not miss having the uvula. Most people describe the pain as similar to a bad viral sore throat that is worse when swallowing. The main risks of uvulectomy are pain, bleeding, and altered speech.
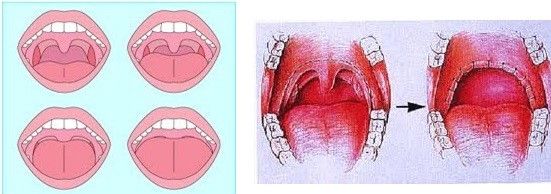
Laser-assisted uvulopalatoplasty (LAUP)
Laser-assisted uvulopalatoplasty (LAUP) involves trimming the palate with a laser. It can be performed under local anaesthesia. Several procedures are usually needed for a maximal effect. The scarring caused by the procedure stiffens the palate, decreasing the ability of the palate to vibrate and pulls the palate sideways to tighten it. The palate can be stiffened by creating scar tissue (as discussed previously) or with implants.
Radio-frequency ablation of the palate
Radio-frequency ablation of the palate can be performed under local anaesthesia. The tissue heals as scar tissue, and the palate becomes stiffer and vibrates less. Generally, scar tissue in the palate continues to form for up to three months. Up to 77% of people report reduced snoring after this procedure, however, as the tissue continues to heal over time, the palate may soften and re-obstruct.
Palate implants
Palate implants are now being used to treat snoring. They are made from Dacron, which is a non-reactive material that has been used for many years for heart valve surgery and hernia repair. Dacron also encourages the normal tissue to grow into it. Small Dacron implants are placed into the palate under local anaesthesia. The implants stiffen the palate like scar tissue after radiofrequency treatments. The implants stay in the tissue, so recurrence of snoring should be reduced.
Obstructive sleep apnea (OSA) is a serious health condition characterized by a repetitive stopping or slowing of breathing that can occur hundreds of times during the night.
A variety of surgical and non-surgical options are available for the treatment of snoring and sleep apnea. In patients having difficulty with other treatments, surgical procedures for the nose and throat can be a beneficial alternative.
Surgery is an effective and safe treatment option for many patients with snoring and sleep apnea, particularly those who are unable to use or tolerate CPAP. Proper patient and procedure selection are critical to the successful surgical management of obstructive sleep apnea. The procedures are done under general anaesthesia, often with overnight hospital observation. Recovery and risks vary depending on the procedure(s) performed but are generally similar to procedures in the upper throat.
- Loud and chronic snoring
- Choking, snorting, or gasping during sleep
- Long pauses in breathing
- Daytime sleepiness, no matter how much time you spend in bed
- Waking up with a dry mouth or a sore throat
- Morning headaches
- Restless or fitful sleep
- Insomnia or nighttime awakenings
- Going to the bathroom frequently during the night
- Waking up feeling out of breath
- Forgetfulness and difficulty concentrating
- Moodiness, irritability, or depression
In many patients with OSA, airway narrowing and collapse occurs in the area of the soft palate (back part of the roof of the mouth), tonsils, and uvula. In general, these procedures aim to enlarge and stabilize the airway in the upper portion of the throat.
The surgery is performed in an operating room under general anaesthesia. The recovery varies depending on the patient and the specific procedures performed. Many patients return to work in approximately one week and return to normal diet and activity at two weeks. Throat discomfort, particularly with swallowing, is common in the first two weeks and usually managed with medications for pain and inflammation. Risks include bleeding, swallowing problems, and anaesthesia complications, although serious complications are uncommon.
The lower part of the throat is also a common area of airway collapse in patients with OSA. The tongue base may be larger than normal, especially in obese patients, contributing to blockage in this area. The tongue may also collapse backwards during sleep as the muscles of the throat relax, particularly when some patients sleep on their back. The epiglottis, or upper part of the voice box, may also collapse and contribute to airway obstruction.
Multiple procedures are available to reduce the size of the tongue base or advance it forward out of the airway. Other procedures aim to advance and stabilize the hyoid bone which is connected to the tongue base and epiglottis. A more recent technique involves implantation of a pacemaker for the tongue (‘hypoglossal nerve stimulator’) which stimulates forward contraction of the tongue during sleep. As with palatal surgery, the most appropriate type of procedure varies from one individual to another and is primarily determined by each patient’s anatomy and pattern of obstruction.
Structural problems, such as a deviated septum and enlarged inferior turbinates often benefit from surgical treatment. One surgical option, known as radiofrequency turbinate reduction uses radiofrequency to shrink swollen tissues in each side of the nose. The tonsils and adenoids may be the sole cause of snoring and sleep apnoea in some patients, particularly children. In children, and in select adults, with OSA and enlarged tonsils/adenoids, tonsillectomy/adenoidectomy alone can provide excellent resolution of snoring, sleep apnoea, and associated symptoms.